Treatment of chronic lymphocytic leukemia (CLL) is rapidly journeying towards yet more new drugs and new combination regimens. Highly encouraging results have been presented over the last years, providing a better prognosis for sub-groups of patients and making CLL a truly exciting field to work in as a researcher. Unfortunately, it seems that all patients have not received a ticket to take part in this voyage. Comorbid and older patients continue to be excluded from most clinical trials, despite representing a substantial proportion of the CLL population (1, 2). Subsequently, treatment decisions for older and comorbid patients in clinical practice are mainly based on efficiency and safety data transferred from younger, fit patients without knowledge of how this corresponds with the sub-group of interest.
In Denmark, we have the worlds’ largest nation-wide cohort of consecutive, unselected patients with CLL (3, 4). This has provided us with a unique opportunity to study and map the impact of individual comorbid conditions on treatment, mortality, and causes of death in patients with CLL. In this study, 9170 patients diagnosed with CLL 1997-2018 were followed, of whom 35% had one ore more comorbid condition of interest.
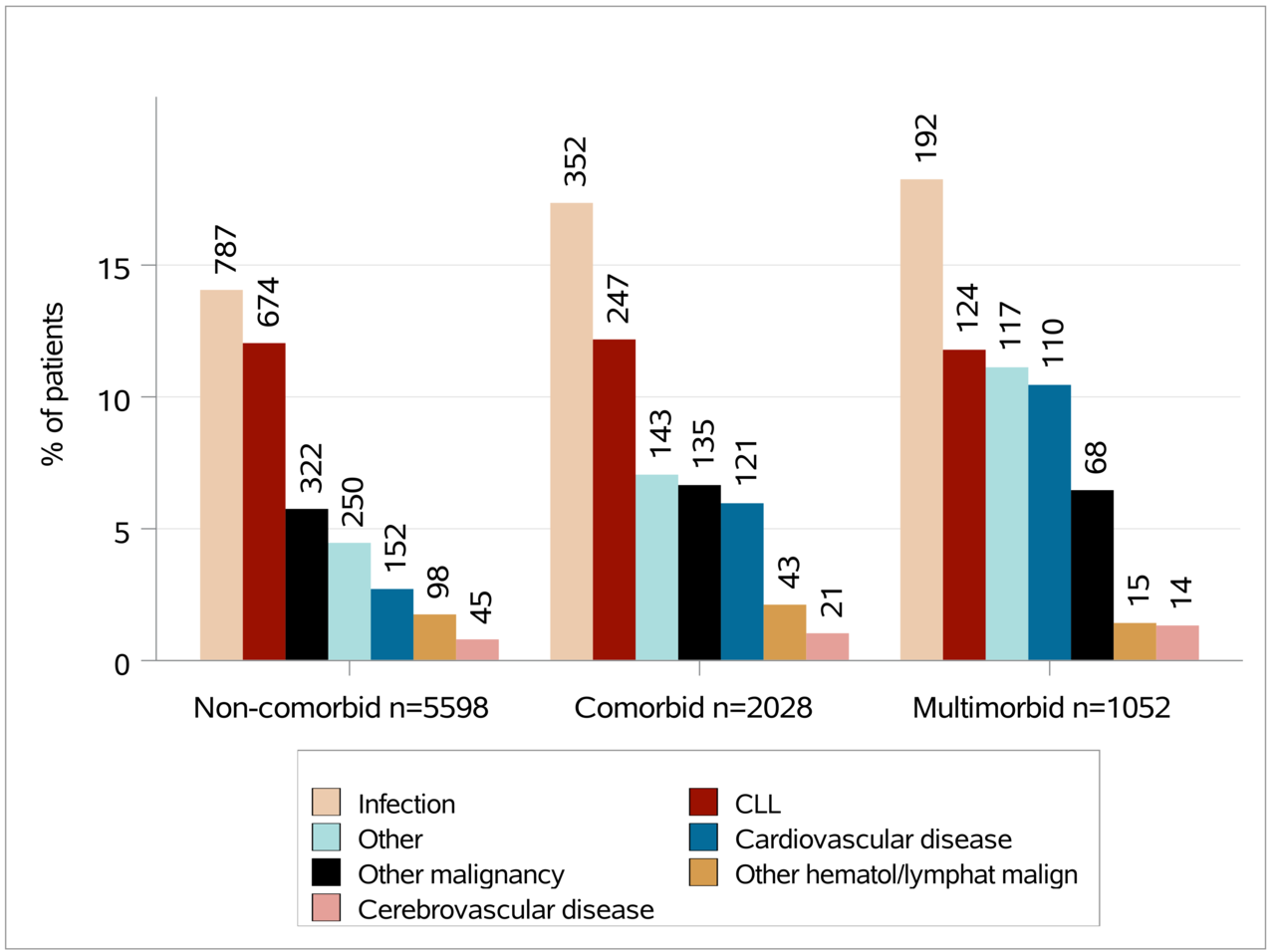
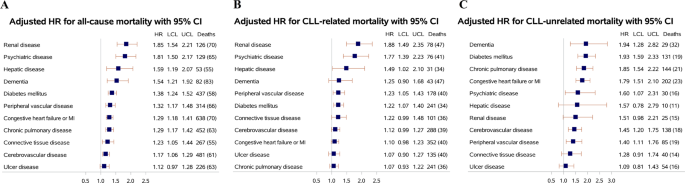
We demonstrate that all comorbid conditions studied were individually associated with increased mortality, and for most conditions also with death related to CLL, including death due to infections and/or malignancies (Figure 1 and 2). Older patients with CLL had a particularly large loss of lifetime compared with the general population. A recent study from our group on major lymphoma sub-types shows promising results even for the oldest patients upon active treatment, stressing that age alone should not be a contraindication for treatment (5).

Our results highlight a large subgroup of CLL patients with an unmet treatment-need and a poor prognosis. Going forward, there is a need for action to improve the outcome for comorbid patients with CLL by prioritizing this sub-group in clinical trials. It is also warranted to investigate interventions that could improve tolerability of treatment in older or comorbid patients with CLL by optimizing geriatric and supportive care. As a scientific and clinical community, it is our responsibility to work towards including all patients with CLL on the incredible journey that is CLL treatment in the 21st century.

Figure 2. Bar chart displaying the distribution of causes of death for patients with CLL from the Danish CLL-register and the Danish Cancer Register who are non-comorbid, comorbid, or multimorbid. N is the number of patients in each sub-group at start of follow-up.
- Klausen TW, Gregersen H, Abildgaard N, Andersen NF, Frølund UC, Gimsing P, et al. The majority of newly diagnosed myeloma patients do not fulfill the inclusion criteria in clinical phase III trials. Leukemia. 2019;33(2):546-9.
- Thurmes P, Call T, Slager S, Zent C, Jenkins G, Schwager S, et al. Comorbid conditions and survival in unselected, newly diagnosed patients with chronic lymphocytic leukemia. Leukemia & lymphoma. 2008;49(1):49-56.
- da Cunha-Bang C, Geisler CH, Enggaard L, Poulsen CB, de Nully Brown P, Frederiksen H, et al. The Danish National Chronic Lymphocytic Leukemia Registry. Clinical epidemiology. 2016;8:561-5.
- Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health. 2011;39(7 Suppl):42-5.
- Wästerlid T, Oren Gradel K, Eloranta S, Glimelius I, El-Galaly TC, Frederiksen H, et al. Clinical characteristics and outcomes among 2347 patients aged ≥85 years with major lymphoma subtypes: a Nordic Lymphoma Group study. British journal of haematology. 2020.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in