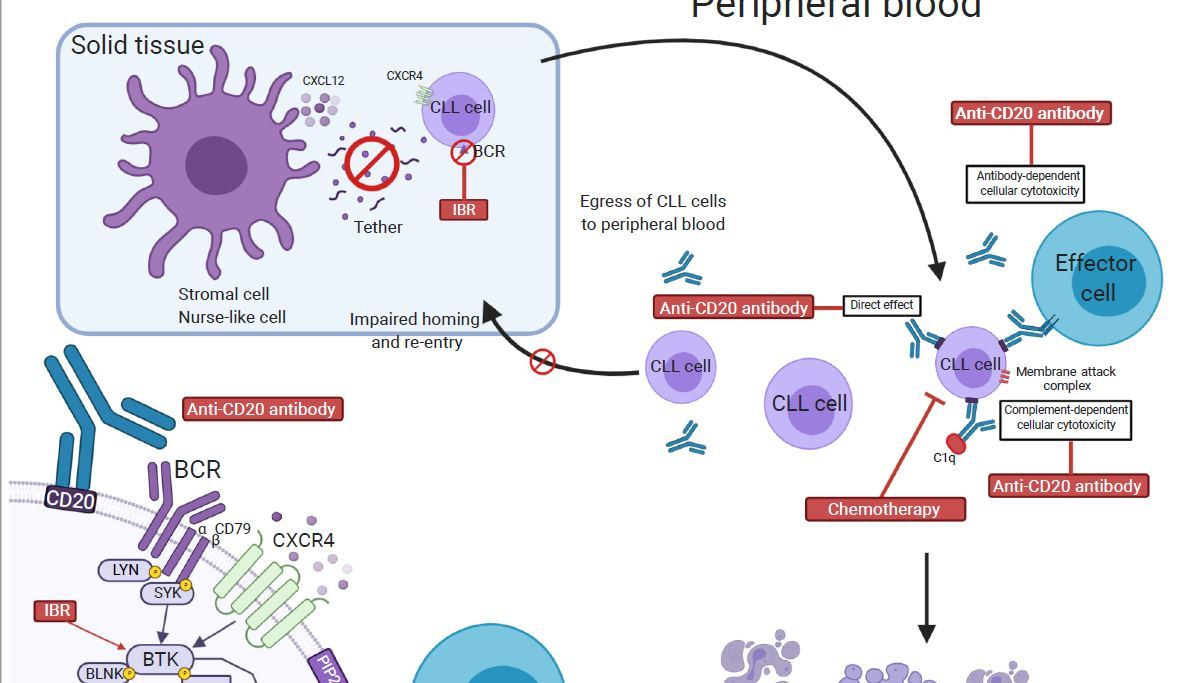
Ibrutinib, because of its efficacy and tolerability has become a drug of choice for patients with chronic lymphocytic leukemia (CLL). However, ibrutinib monotherapy has four significant limitations; low rate of complete remission (CR), development of resistance, cumulative off-target toxicity, and high treatment cost due to prolonged use. Targeting different elements of CLL pathophysiology using combination therapy is a promising option to overcome these obstacles (Figure 1) and to augment the rate of CR with undetectable minimal residual disease (uMRD).

In our review,1 we have summarized four relevant directions of ibrutinib combination strategies: with anti-CD20 monoclonal antibodies, with chemoimmunotherapy, with cell therapy, and with targeted agents.
Combinations of ibrutinib and anti-CD20 antibodies were first to be investigated. While in the head-to-head comparison, the addition of rituximab to ibrutinib did not improve survival outcomes in patients with CLL,2 the next generation of anti-CD20 monoclonal antibodies (obinutuzumab and ofatumumab) have different interactions with ibrutinib and show promising outcome with clinically meaningful endpoints such as progression-free and overall survival.3,4 Obinutuzumab and ibrutinib couplet demonstrated the feasibility of a time-limited treatment based on MRD status after the induction therapy.5 MRD-negative patients in CR represent a favorable group of patients for a fixed-duration treatment with ibrutinib combinations.
Chemoimmunotherapy is cost-effective and of short-duration making it a desired treatment option especially for fit patients. The addition of ibrutinib to the standard of care chemoimmunotherapy improves survival outcomes and increases the number of deeper responses.6-8 Additionally, concomitant ibrutinib administration gives an opportunity to reduce the dose or the number of chemoimmunotherapy cycles, thereby potentially decreasing chemotherapy-associated adverse effects.9
Chemotherapy-resistant CLL has become a critical challenge for treatment. While at an early stage, CAR-T cell therapy becomes a hopeful option for these cohorts of patients to achieve a response. Studies showed that patients, who receive ibrutinib prior to CAR-T cell therapy have better chimeric CTL019 cells proliferation and survival, and milder manifestations of the cytokine release syndrome.10,11 Novel cell therapy strategies are being tested with concomitant ibrutinib administration.
The most promising and patient- and physician-preferred option for CLL treatment is chemo-free targeted therapy combinations. The new trend of a fixed-duration treatment was incorporated into a combination of ibrutinib with venetoclax.12 Patients with CR and u-MRD become candidates for time-limited treatment, potentially reducing ibrutinib resistance, untoward toxicities with continuous use, and treatment cost for private and governmental payers. This approach shows encouraging preliminary results with a low rate of relapse after therapy discontinuation. The UK CLARITY study13 has shown that not only the MRD status is important for a favorable outcome, but the velocity of attaining a remission is highly predictive of long-term response. Early data from studies of ibrutinib with venetoclax show deep responses resulting in a high rate of CR and u-MRD.12-15 More forthcoming studies of ibrutinib or the next generation of irreversible and reversible BTK inhibitors in combination with other targeted drugs and monoclonal antibodies will provide more definite answers. For the first time, there is an optimism of chemo-free yet short-duration therapy of CLL.
1 Timofeeva, N. & Gandhi, V. Ibrutinib combinations in CLL therapy: scientific rationale and clinical results. Blood Cancer Journal 11, 79, doi:10.1038/s41408-021-00467-7 (2021).
2 Burger, J. A. et al. Randomized trial of ibrutinib vs ibrutinib plus rituximab in patients with chronic lymphocytic leukemia. Blood 133, 1011-1019, doi:10.1182/blood-2018-10-879429 (2019).
3 Jaglowski, S. M. et al. Safety and activity of BTK inhibitor ibrutinib combined with ofatumumab in chronic lymphocytic leukemia: a phase 1b/2 study. Blood 126, 842-850, doi:10.1182/blood-2014-12-617522 (2015).
4 Moreno, C. et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial. The Lancet Oncology 20, 43-56, doi:10.1016/s1470-2045(18)30788-5 (2019).
5 Michallet, A. S. et al. Obinutuzumab and ibrutinib induction therapy followed by a minimal residual disease-driven strategy in patients with chronic lymphocytic leukaemia (ICLL07 FILO): a single-arm, multicentre, phase 2 trial. Lancet Haematol 6, e470-e479, doi:10.1016/s2352-3026(19)30113-9 (2019).
6 Brown, J. R. et al. The Bruton tyrosine kinase inhibitor ibrutinib with chemoimmunotherapy in patients with chronic lymphocytic leukemia. Blood 125, 2915-2922, doi:10.1182/blood-2014-09-585869 (2015).
7 Chanan-Khan, A. et al. Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double-blind, phase 3 study. The Lancet Oncology 17, 200-211, doi:10.1016/s1470-2045(15)00465-9 (2016).
8 Davids, M. S. et al. Ibrutinib plus fludarabine, cyclophosphamide, and rituximab as initial treatment for younger patients with chronic lymphocytic leukaemia: a single-arm, multicentre, phase 2 trial. Lancet Haematol 6, e419-e428, doi:10.1016/s2352-3026(19)30104-8 (2019).
9 Jain, N. et al. Ibrutinib, Fludarabine, Cyclophosphamide, and Obinutuzumab (GA101) (iFCG) for First-Line Treatment of Patients with CLL with Mutated IGHV and without TP53 Aberrations. Blood 130, 495-495, doi:10.1182/blood.V130.Suppl_1.495.495 (2017).
10 Long, M. et al. Ibrutinib treatment improves T cell number and function in CLL patients. J Clin Invest 127, 3052-3064, doi:10.1172/JCI89756 (2017).
11 Gauthier, J. et al. Feasibility and efficacy of CD19-targeted CAR T cells with concurrent ibrutinib for CLL after ibrutinib failure. Blood 135, 1650-1660, doi:10.1182/blood.2019002936 (2020).
12 Tam, C. S. et al. Ibrutinib (Ibr) Plus Venetoclax (Ven) for First-Line Treatment of Chronic Lymphocytic Leukemia (CLL)/Small Lymphocytic Lymphoma (SLL): Results from the MRD Cohort of the Phase 2 CAPTIVATE Study. Blood 134, 35-35, doi:10.1182/blood-2019-121424 (2019).
13 Hillmen, P. et al. Ibrutinib Plus Venetoclax in Relapsed/Refractory Chronic Lymphocytic Leukemia: The CLARITY Study. J Clin Oncol 37, 2722-2729, doi:10.1200/jco.19.00894 (2019).
14 Jain, N. et al. Ibrutinib and Venetoclax for First-Line Treatment of CLL. N Engl J Med 380, 2095-2103, doi:10.1056/NEJMoa1900574 (2019).
15 Jain, N. et al. Combined Ibrutinib and Venetoclax in Patients with Relapsed/Refractory (R/R) Chronic Lymphocytic Leukemia (CLL). Blood 134, 359-359, doi:10.1182/blood-2019-131732 (2019).




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in