For many years, primary tumour location has become an interesting and useful marker to predict the prognosis in patients with colorectal cancer. According to the subgroup analysis of CALGB/SWOG 80405 and FIRE-3 studies, sidedness seems be the one of the most important predictive markers in treating mCRC with bioagents. Both of NCCN and ESMO/Pan-Asian guidelines point out that a cytotoxic doublet plus an EGFR antibody should be the preferred treatment in patients with left-sided colon cancer, whereas bevacizumab-based therapy is limited to the group of patients with right-sided colon cancer.
However, in our daily clinical practice and weekly multidisciplinary team discussion, we found that the efficacy of anti-EGFR therapy in treating metastatic colorectal cancer seems different between rectum and left-sided colon.
In Taiwan, Medical oncologists adapted the current international consensus and followed the treatment principles for mCRC. However, the National Health Insurance does not reimburse the cost of anti-VEGF treatment as non-first-line therapy once first-line anti-EGFR treatment fails, regardless of the primary tumour location. Therefore, in left-PTL cases, after shared decision making with the patients, some of them still choose anti-VEGF-based treatment initially because of their financial situation, although it might be against current Pan-Asian adapted ESMO guidelines. Owing to this special reimbursement policy, our multidisciplinary team had a chance to collect more comprehensive data (anti-EGFR as post-VEGF therapy for RAS-wt, left-sided colon cancer), to compare the different bioagent treatment sequences, and eventually to determine that the efficacy of anti-EGFR was lower for middle/low rectal cancer than for left-sided colon cancer.
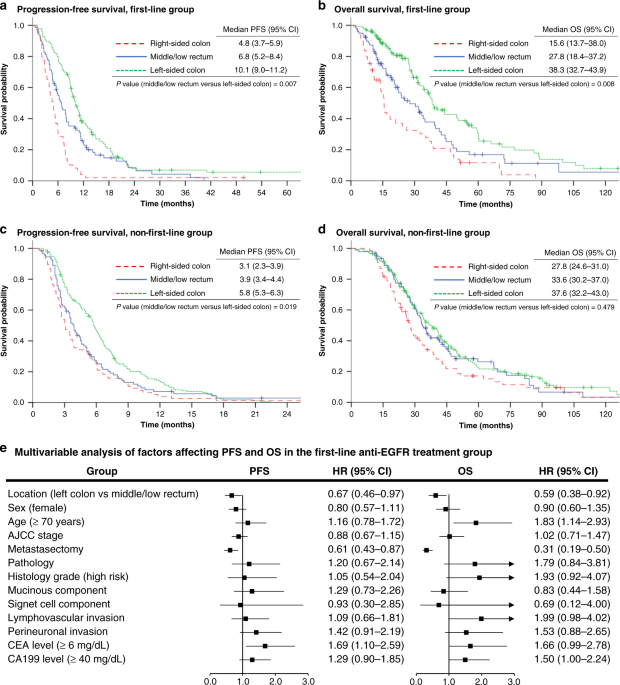
According to the latest ESMO guidelines, rectal cancer is divided into high, middle, and low rectal cancer (>10 to 15 cm, ≥5 to 10 cm, and <5 cm from the anal verge, respectively). However, some results have suggested that high rectal tumours have similar characteristics to left-sided CRC, including different lymphatic drainage and vascular supply systems, distinguishing metastatic patterns, response to adjuvant chemotherapy, and even survival outcomes. Whether tumours located 10 to 15 cm from the anal verge should be defined as colon or rectal tumours is still under debate. In our research, we provided evidence that there are differential treatment outcomes between metastatic left-sided colon and middle/low rectal cancers under anti-EFGR treatment. In terms of the first-line anti-EGFR therapy group, PFS, OS, and ORR were significantly higher in the left-sided CRC group than in the middle/low rectal tumour group. Significantly longer PFS and DCR were also observed in patients with left-sided tumours compared to middle/low rectal tumours under non-first-line anti-EGFR therapy.
To validate our clinical findings, “TCGA Pan-Cancer Atlas” project on the cBioPortal TCGA website was utilized to explore the differential expression of genomic features among left-, right-sided colon, and rectal cancer. The data were analysed in different levels, including single nucleotide polymorphisms (SNPs), the transcriptome (mRNA), and DNA methylation. The results serve some possible explanations that the rectum is not substantially identical to the left-sided colon. Conversely, rectal cancers show features resembling those of both left- and right-sided colon cancers.
In short, this article may be the first one comparing the efficacy among metastatic middle/low rectal cancer with left-sided colon cancer under both first-line and non-first-line settings. If you are interested in this topic, we encourage you to find more details in our full-text publication on British Journal of Cancer website. Again, we hope our findings will serve as an act of “tossing a stone to find out what's ahead”, attracting the attention of specialists and scholars to this relevant topic.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in